
Share On Social!
This is part of the “Advancing the Science of Cancer in Latinos: 2022 Conference Proceedings,” which summarizes findings and discussions of the 2022 Advancing the Science of Cancer in Latinos Conference on Feb. 23-25, 2022, in San Antonio, Texas.
Updates in Genomics of Breast Cancer among Latina Women
Dr. Elad Ziv is a Professor of Medicine at the University of California San Francisco (UCSF), with a research focus on human genetics of cancer susceptibility and hematological traits.
Genomics explained

To set the stage for his presentation, Dr. Ziv explained genomics in a lay-friendly way, describing it as a long series of letters. A change of one letter in this series, from an A to a G for example, can lead to anything from a change in height to a disease susceptibility. Not all pages of the “book” of genomics are understood, and there are portions of the genome that are still a mystery, so there is an aspect of careful deciphering involved each time a new individual is sequenced.
In the context of cancer, there are two types of genetic variation. The first is inherited genetic variation. This variation involves mutations in genes which can be passed down within families, which affect all cells, and which can affect disease susceptibility. The second is somatic genetic variation. This variation involves mutations in a small subset of cells, cannot be passed on from parent to child, and can sometimes lead to abnormal growth or cancer.
Insights from the Romero-Cordoba study
Until recently there has been very little research concerning somatic genetic variation in Latinas. One study by Romero-Cordoba and colleagues from the Mexican National Institute of Genomic Medicine found that 28% of Hispanic-Mexican women with breast cancer had a mutation in a gene called PIK3CA. This gene is commonly mutated in other populations as well, and it encodes a protein that is commonly targeted by anti-cancer therapies. The second most commonly mutated gene in Hispanic-Mexican women, TP53, is also common in breast cancer in other populations. However, the third most commonly mutated gene, AKT1, does not typically play a role in other populations. The fact that this gene encodes a protein that can be targeted by anti-cancer therapies makes it worthy of further study. Although Dr. Ziv’s own work has not yet corroborated this elevated AKT1 mutation prevalence in the Latina population, research is ongoing in this area.
A new look at breast cancer in Latinas
In Dr. Ziv’s lab, 147 tumors from 141 Latina women were sequenced. The mean age of the cohort was 48.7 years, and most cancers were stage I and II, with only 14% being stage III or IV. Most tumors (82%) were estrogen receptor (ER) positive, and 71% were progesterone receptor (PR) positive. About 17% were human epidermal growth factor receptor (HER2) positive, a higher proportion than in the general population. Dr. Ziv compared his cohort with The Cancer Genome Atlas (TCGA) program, a large, publicly available genomic database that unfortunately has a very low number of Latina women.
Comparing somatic mutational signatures
In comparing the two cohorts, Dr. Ziv considered somatic mutational signatures, which look not only at individual mutations, but at common mutational patterns. Signatures 2 and 13, for example, are associated with an APOBEC mutational pattern, which is seen in breast cancer and other cancers. Signature 3 is associated with a homologous recombination repair defect that prevents cells from repairing double stranded DNA. All three of these signatures were found at similar rates in the Latina cohort and TCGA.
A new signature was found, however, that had not previously been reported in association with breast cancer. This new finding, signature 16, was amplified in two breast cancer subtypes, luminal A and luminal B, and was found to be more common in Latinas compared with non-Hispanic White patients. Signature 16 represented 27% of the Latina cohort in Dr. Ziv’s work, and 20% of Latinas in the Romero-Cordoba study. However, signature 16 was only found in 10% of non-Hispanic White patients from TCGA.
Comparing genetic composition through copy number analysis
Another difference between the Latina cohort and TCGA was found through copy number analysis. Many tumors not only have mutations, but also amplify certain parts of the genome, which can be assessed through copy number analysis. In Dr. Ziv’s Latina cohort, a gene called KIA0100 was found to have high amplification and high gene expression in 11 women. This was compared to zero women in the entire TCGA dataset.
In summary, Dr. Ziv emphasized the key findings from his work. First, signature 16, which is more commonly associated with luminal cancers, is more prevalent in Latinas. Second, although Dr. Ziv’s findings have yet to corroborate the finding, the Romero-Cordoba study shows a higher rate of AKT1 mutations in Latinas, representing an important area for future study. Finally, there is higher amplification and expression of the KIA0100 gene in Latina women.
Updates and Trends in Breast Cancer Treatment: Advancing the Science of Cancer in Latinos
Dr. Filipa Lynce is Assistant Professor of Medicine at the Dana-Farber Cancer Institute at Harvard Medical School.
Breast cancer in Hispanic women

Breast cancer is the most commonly diagnosed cancer, as well as the leading cause of cancer death among Hispanic women. Although incidence of breast cancer in Hispanic women remains about 29% lower than in non-Hispanic White women, the rate increased by about 0.4% annually from 2006 to 2015, while it has remained stable in non-Hispanic White women. Mortality rates have been decreasing; however, the rate of decrease is 1.1% per year in Hispanic women versus 1.8% per year in non-Hispanic White women. Breast cancer is also less likely to be diagnosed at the localized stage in Hispanic women, with only 57% compared with 65% in non-Hispanic White women.
In the general population, 68% of breast cancer patients present with the hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-) subtype, 10% have HR-/HER2-, 10% have HR+/HER2+, 4% have HR-/HER2+, and 7% are unknown. Hispanic women, however, are more likely to be diagnosed with HR-/HER2+ and HR-/HER2- tumors. The latter, also called triple negative breast cancer (TNBC), affects Hispanic women at a rate of 16-17% compared with 11-15% for non-Hispanic White women. Both HR-/HER2+ and TNBC are associated with worse outcomes.
Novel therapies for breast cancer
Dr. Lynce presented five novel therapies recently approved for breast cancer. The first was immunotherapy, and pembrolizumab is currently the only immunotherapy drug approved for the treatment of breast cancer. Importantly, pembrolizumab is approved for the treatment of high-risk, early-stage TNBC, showing improvement in event-free survival (EFS) in early stages and overall survival (OS) in advanced settings when compared with chemotherapy alone. It is associated with some immune-related adverse events (irAEs), including skin conditions, gastrointestinal (GI) pathologies, and endocrinopathies.
Poly-ADP ribose polymerase (PARP) inhibitors represent another novel therapy for breast cancer treatment. Two therapies in this drug class, olaparib and talazoparib, have been approved for the treatment of HER2- breast cancers. Olaparib has shown improvement in disease-free survival (DFS) in the adjuvant setting in patients with high-risk, early-stage, HER2- breast cancer. The main toxicities are anemia, neutropenia, nausea, vomiting, and fatigue.
Another novel therapy involves antibody-drug conjugates, also called “smart bombs” due to their ability to deliver large doses of chemotherapies directly to tumors through linkage to specific antibodies. Two drugs that received recent approval are sacituzumab govitecan and trastuzumab deruxtecan. Sacituzumab govetican has been approved for the treatment of metastatic TNBC, and showed improvement in progression-free survival (PFS) and OS compared to chemotherapy. Trastuzumab deruxtecan has been approved for the treatment of stage IV HER2+ breast cancer.
Tyrosine kinase inhibitors are yet another novel approach to breast cancer treatment. Tucatinib, an oral chemotherapy agent, has been approved in combination with trastuzumab and capecitabine for the treatment of metastatic HER2+ breast cancer. It is also the first drug to show significant activity against active CNS disease.
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors were the final novel approach presented by Dr. Lynce. Three of these inhibitors have been approved for the treatment of HR+/HER2- breast cancer. Palbociclib and ribociclib have been approved in combination with endocrine therapy in the metastatic setting, showing improved PFS compared to endocrine therapy alone. Abemaciclib has been approved for the adjuvant treatment of node-positive early breast cancer at high risk of recurrence and metastatic HR+/HER2- breast cancer.
Unique challenges for novel therapies in the Hispanic community
Despite the promise of these novel therapies, questions and challenges specific to the Latino population remain. In immunotherapy, for example, there is insufficient data to determine whether differences exist between racial and ethnic groups on dosing, efficacy, and adverse events. When it comes to PARP inhibitors, there may be a lower number of Latinas eligible due to a lower uptake of genetic testing in the Latino population. In the pivotal sacituzumab study, which is one of the antibody-drug conjugates, the median duration of treatment was lower in Latinos compared with White patients. Finally, since the Latino population has been shown to have lower adherence to oral medications due to concerns with side effects as well as copays, therapies involving tyrosine kinase inhibitors and CDK4/6 inhibitors might be affected.
Dr. Lynce closed by stressing the disparity of Latinos represented in clinical trials. Despite representing 18% of the population, Latinos only represent 4-8% of clinical trial participants. In a recent study of almost 6000 precision oncology trials, all minority groups were underrepresented, with Latinos showing the greatest disparity.
The Landscape of Breast Cancer Genetics in Puerto Rico
Dr. Julie Dutil leads the Cancer Genetics & Genomics Research Program at the Ponce Research Institute at Ponce Health Sciences University in Ponce, Puerto Rico.
The importance of understanding genetic uniqueness

Dr. Dutil began by stressing the importance of genetic uniqueness in the realm of health and disease risk. However, genome-wide association studies (GWAS) show great disparity in cancer study representation, with Latin American patients accounting for only about 1% of participants. The Cancer Genome Atlas (TCGA) also shows underrepresentation, with only 3% of participants identifying as Hispanic or Latino. Even in laboratory research of cellular models of cancer, cellular lines originating from White or Asian patients are easily available, while African or Hispanic samples are more difficult to obtain.
Hispanic populations are admixed, meaning they originated from three different sources: Indigenous American, European, and African populations. Hispanic populations are therefore heterogeneous, and genetic components vary by area. The Mexican population, for example, has a larger Indigenous American component than the Puerto Rican population, which has a larger African component. Even within the Puerto Rican population genetic components vary, with residents in areas that were formerly sugar cane plantations having a stronger African genetic component.
The Puerto Rico Breast Cancer Genetics and Genomics Study
In order to assess how these genetic variations affect breast cancer risk, Dr. Dutil started the Puerto Rico Breast Cancer Genetics and Genomics Study (PUR-BCGG) in Ponce, Puerto Rico. In this study, both breast cancer patients and non-cancer controls were recruited from oncology practices, surgery practices, family medicine clinics, and community events. The study began as a hereditary cancer screening and has grown into a large biobank of almost 2000 participants with a wealth of information on each patient, including blood samples, pathology reports, family history, demographics, tumor formalin-fixed paraffin-embedded (FFPE) blocks, and ongoing 5-year follow-up data on recurrence and survival.
Founder and bottleneck effects in Puerto Rico
A principle component analysis of the Puerto Rican cohort showed varied heredity, with some participants showing strong European ancestry and others strong African ancestry. The cohort also showed founder and bottleneck effects, with individuals sharing longer chromosome segments than what is found in other populations. This results in a higher frequency of rare syndromes such as Hermansky Pudlack Syndrome types 1 and 3 (HPS-1 and HPS-3), due to a European founder effect, and Steel Syndrome (COL27A1), due to a bottleneck event in the Indigenous American population. For most populations, prevalence of all types of HPS is 1/500,00 to 1/1,000,000; however, in Northwest Puerto Rico, HPS-1 has a prevalence of 1/1800. Steel Syndrome, a collagen mutation associated with short stature, scoliosis, and dislocation problems, is almost absent from the rest of the world, but is relatively common in Puerto Rico.
A founder effect is also observed among cancer patients in Puerto Rico, where BRCA2 mutations occur at a higher rate than in the rest of the world. Roughly 70% of breast cancer patients with a BRCA2 mutation were found to carry the E1308X mutation, which originates from Europe. These individuals had a large, shared haplotype, indicative of founder effect. In many US-based Hispanic studies the pathogenic variants that are identified are similar to those found in Mexican studies, indicating a possible bias in the literature toward Hispanic or Latino research with Mexican origin compared to other countries.
Outcomes associated with African Ancestry
Using PUR-BCGG, Dr. Dutil also looked at whether the polygenic risk scores (PRS) used for predicting breast cancer risk could be applied in Puerto Rico, excluding BRCA mutation carriers or high-risk carriers. Populations that were very low in African ancestry but high in European ancestry were compared to populations that were fourth quartile African ancestry. Interestingly, PRS scores were found to be diminished as African ancestry increased.
African ancestry, however, was found to carry increased risk of triple negative breast cancer. To understand this trend, Dr. Dutil assessed the Puerto Rican cohort to identify sites in the genome that control that increased risk. Using mixture mapping, which involved looking at enrichment of certain ancestries in cases versus control, a site was found in triple breast negative cancer patients on chromosome 14 which was enriched for African ancestry. Fine mapping of that region showed two genes of interest, which are the focus of ongoing study.
To conclude, Dr. Dutil summarized the results of her work. First, a higher ratio of BRCA2 to BRCA1 mutations was observed in Puerto Rico, which has implications in the clinical management of cancer risk in carrier families. European founder BRCA2 E1308X was the predominant pathogenic variant in this population. The architecture of breast cancer genetic risk may differ between Hispanic/Latino populations of different origins, with unique variants and altered frequencies in each population. Finally, a better understanding of the genetic basis to cancer susceptibility must be pursued as a key component for eliminating cancer health disparity.
Lung Cancer in Latinos: Disparities Across the Continuum of Care
Dr. M. Patricia Rivera is a Professor of Medicine and Chief of the Division of Pulmonary and Critical Care Medicine at the University of Rochester in Rochester, New York.
Lung cancer in the United States

To set the stage for her presentation, Dr. Rivera began by explaining the magnitude of the burden of lung cancer in the United States. Lung cancer is the leading cause of cancer deaths in the US in both men and women.1 It is also the leading cause of cancer deaths in Latino men in the US and is second to breast cancer in Latino women.1 Black men and women, Native Hawaiians, Latino women, and White women have a higher risk of lung cancer at a younger age and lower smoking exposure.2,3 In cancer care, socioeconomic status is associated with more significant disparities than racial or ethnic factors, and lung cancer is the disease most affected by socioeconomic factors.4
Latino men and women have lower smoking rates than White men and women, 12% versus 16% and 6% versus 16%, respectively.5 That being said, smoking rates among Latino women vary widely by geographical location, with 6% of Central Americans smoking compared to 17% of Puerto Ricans.5 While Latino high school students smoke at about the same rate as White students, Latino middle school students have higher smoking rates, at 9% compared to 6% for White students.5 This may be due to tobacco companies targeting minorities and individuals of low-socioeconomic status. Low-income neighborhoods with a higher percentage of Blacks and Latinos have higher numbers of tobacco retailers. There are also more tobacco retailers near schools in low-income neighborhoods.6,7
The Hispanic paradox
Latino men and women have much lower incidences of lung cancer and mortality than Black or White men and women.8 However, Latinos are more likely to be diagnosed with advanced-stage lung cancer9, more likely to have low socioeconomic status and treatment delays, and less likely to be insured and have access to lung cancer screening. This juxtaposition of lower mortality paired with high-risk factors describes the Hispanic paradox in lung cancer.10
Possible factors contributing to the lung cancer survival advantage among Latinos are many. The lower prevalence of smoking could play a role, as well as the higher incidence of adenocarcinoma, which has a better prognosis. Higher rates of EGFR mutations and lower rates of KRAS mutations are possible factors, along with dietary habits, community support, genetics, and selective migration.10 The whole picture is unclear because much of the knowledge describing lung cancer in Latinos is missing.
The importance of lung cancer screening
Lung cancer screening is one of the most critical interventions for decreasing lung cancer mortality, second only to smoking prevention and cessation. Patients who undergo early screening are much more likely to be diagnosed with stage I disease, which is curable. However, the National Lung Screening Trial (NLST), the largest randomized trial in the history of lung cancer screening, comprised more than 90% of White participants.11
In 2021 the United States Prevention Services Taskforce (USPSTF) lowered its recommended age for lung cancer screening to adults aged 50 to 80 with a 20-pack-year smoking history.12 This represents 14.5 million people eligible for lung cancer screening, an 87% increase over the 2013 recommendations and a 112% increase in eligible Hispanics.13 Despite these gains, eligibility-to-incidence ratios are still higher in White populations than in Hispanics.14 This is partially due to a low number of screening centers in areas with high Hispanic populations.15
Cessation of smoking in the Hispanic community
When considering smoking cessation, Hispanics are more motivated to quit than their White and Black counterparts.16 However, they have limited access to cessation medication and support services. Only 42.2% of Hispanics have access to physician advice, compared to 60.2% for White individuals and 55.7% for Black individuals.16 A lower percentage of Hispanics have access to counseling than White and Black individuals (5.1% vs. 6.9% and 7.6%, respectively). Further, only 16.6% of Hispanics receive pharmacotherapy compared to 32.6% for White individuals and 25% for Black individuals.16
Hispanic involvement in clinical trials
Although immunotherapy has revolutionized the treatment of advanced stages of lung cancer, very few Hispanics have been enrolled in clinical trials, representing only 3% of clinical trial participants.17,18 When comparing participants in clinical trials from 1996-2002 with participants from 2003-2016, Hispanic and Black participation has decreased, with 3.1% Hispanic participation before 2002 compared with 2.6% participation after 2003.17,18
To close, Dr. Rivera discussed strategies to help overcome healthcare disparities in lung cancer. Increasing access to healthcare, recruiting minority physicians, building trust through communication, providing education, using nurse/patient navigators, and involving communities are all critical approaches. Tailoring strategies to each culture and providing cultural competency training is also imperative. With these interventions, the burden of disparity in lung cancer can be lessened, and more equitable healing can begin.
References
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33.
- Stram DO, Park SL, Haiman CA, et al. Racial/ethnic differences in lung cancer incidence in the Multiethnic Cohort study: an update. J Natl Cancer Inst. 2019;111(8):811-819.
- Jemal A, Miller KD, Ma J, et al. Higher lung cancer incidence in young women than young men in the United States. N Engl J Med. 2018;378(21):1999-2009.
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011;61(4):212-236.
- Gentzke AS, Wang TW, Cornelius M, et al. Tobacco product use and associated factors among middle and high school students – National Youth Tobacco Survey, United States, 2021. MMWR Surveill Summ. 2022;71(5):1-29.
- Seidenberg AB, Caughey RW, Rees VW, et al. Storefront cigarette advertising differs by community demographic profile. Am J Health Promot. 2010;24(6):e26.
- Aspire Center. Retail tobacco density & access. Accessed October 14, 2022. http://aspirecenter.org/wp-content/uploads/2020/08/ASPiRE_RetailTobaccoDensityandAccess_ExecSumm.pdf
- NIH. SEER cancer stat facts: cancer disparities. Accessed October 14, 2022. https://seer.cancer.gov/statfacts/html/disparities.html
- American Cancer Society. Cancer facts and figures for Hispanic/Latino people 2021-2023. Accessed February 3, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-hispanics-and-latinos/hispanic-latino-2021-2023-cancer-facts-and-figures.pdf
- Kumar R, Castillero F, Bhandari S, et al. The Hispanic paradox in non-small cell lung cancer. Hematol Oncol Stem Cell Ther. 2021:S1658-3876(21)00029-7.
- National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395-409.
- US Preventive Services Task Force, Krist AH, Davidson KW, Mangione CM, et al. Screening for lung cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962-970.
- Meza R, Jeon J, Toumazis I, et al. Evaluation of the benefits and harms of lung cancer screening with low-dose computed tomography: modeling study for the US Preventative Services Task Force. JAMA. 2021;325(10):988-997.
- Pinsky PF, Lau YK, Doubeni CA. Potential disparities by sex and race or ethnicity in lung cancer screening eligibility rates. Chest. 2021;160(1):341-350.
- Kale MS, Wisnivesky J, Taioli E, et al. The landscape of US lung cancer screening services. Chest. 2019;155(5):900-907.
- Babb S, Malarcher A, Schauer G, Asman K, Jamal A. Quitting smoking among adults – United States, 2000-2015. MMWR Morb Mortal Wkly Rep. 2017;65(52):1457-1464.
- Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: race-, sex-, and age-based disparities. JAMA. 2004;291(22):2720-2726.
- Duma N, Vera Aguilera J, Paludo J, et al. Representation of minorities and women in oncology clinical trials: review of the past 14 years. J Oncol Pract. 2018;14(1):e1-e10.
Targeting Tumor Microenvironments in Lung Cancer
Dr. Josephine Taverna is Assistant Professor in the Division of Hematology Oncology in the Department of Medicine with a joint appointment in the Department of Molecular Medicine at the University of Texas Health Science Center.
The poor prognosis of lung cancer

In clinical practice Dr. Taverna treats lung cancer patients, approximately 50% of whom are Hispanic. Unfortunately, many of her patients present with advanced-stage lung cancer, which has a poor prognosis. Chemotherapy alone is associated with a 5-year overall survival of 5%, while recent advances in immunotherapy have increased that number to 24%. Clearly, novel therapies are needed to improve survival.
The AXL signaling pathway and the STAT3 bypass
One pathway that plays an important role in tumor biology is the AXL signaling pathway, which is upregulated in many tumors, including lung cancer tumors. This pathway triggers other oncological pathways, creating resistance not only to chemotherapy and immunotherapy but also to targeted drugs such as EGFR and ALK inhibitors. To make matters worse, it also pushes the tumor to metastasize.
In order to further understand how the AXL pathway works, Dr. Taverna and colleagues analyzed 50 tumors for high AXL versus low AXL expression. Tumors that metastasized were found to have high AXL expression, while stage I and II tumors were found to have low but increasing AXL expression. Accordingly, when AXL was inhibited, tumor growth was slowed.
AXL inhibition alone, however, proved to be insufficient in completely halting tumor growth and proliferation. When blocking the AXL pathway, many oncological pathways were inhibited as expected; however, a bypass mechanism was discovered called STAT3. The STAT3 pathway became amplified when the AXL pathway was blocked and continued to drive tumor growth and alter the tumor microenvironment despite AXL inhibition. The implication of this bypass is that an AXL inhibitor alone would be insufficient for tumor treatment.
Macrophages in the tumor microenvironment
To understand AXL and STAT3 on a deeper level, Dr. Taverna undertook tumor ecosystem single cell profiling for the first 15 tumors, which meant exploring the entire tumor microenvironment: tumor cells, immune cells, macrophages, stromal cells, endothelial cells, and more. In the more aggressive tumors, it became clear that the AXL and STAT3 pathways were upregulated not only in the tumor cells, but in other cells as well, including macrophages. In fact, tumor cells and macrophages were found to have a mutual dependency which was strengthening the cancer.
When tumors begin, they typically have macrophages that act against them, activating T-cells or phagocytizing the tumor cells. After the AXL and STAT3 pathways are amplified, however, macrophages are recruited and polarized from M1 to M2 macrophages. The M2 macrophages then work with the tumor to suppress the immune system and initiate angiogenesis for the tumor’s benefit.
Testing AXL-STAT3 inhibitors
To test drug efficacy against these tumors, organoids were grown to replicate tumors, which were then treated ex vivo. Organoids that showed high AXL/STAT3 signaling (measured with cytometry time of flight (CyTOF)) were treated with AXL/STAT3 inhibitors. Response by the organoid to this inhibition indicates the patient may respond to this type of treatment regimen and should be enrolled in a clinical trial. This is the future of personalized lung cancer treatment.
One patient, for example, a 57-year-old female who smoked heavily, had low expression of AXL and STAT3. Accordingly, when her organoid tumor was treated with an AXL and STAT3 inhibitor, little improvement was noted. However, when treating an organoid from a patient with an aggressive tumor, which exhibited high AXL and STAT3 expression, the organoid tumor responded very well to inhibitor therapies.
The astounding effects of AXL-STAT3 inhibition
The A549 lung cancer xenograft mouse model was then used to test this theory. Treating these mice with a JAK inhibitor had no effect, treating with an AXL inhibitor had some effect, but combining the two produced the strongest outcome of tumor growth inhibition. In fact, the combined JAK/STAT3 inhibition actually dismantled the tumor microenvironment and there was an M2 to M1 shift in the macrophages. In fact, when tumors were treated with both AXL and STAT3 pathway inhibitors, the entire tumor microenvironment was affected. Macrophages not only decreased, but actually shifted from M2 back to M1. Recruitment of other cells was also interrupted, including fibroblasts, endothelial cells, natural killer cells, B lymphocytes, and T lymphocytes.
In concluding her presentation, Dr. Taverna promoted the personalized approach as the future of cancer therapy. In contrast with chemotherapy, which attempts to kill tumor cells with little regard for the patient’s experience, this approach allows clinicians to select targeted therapies that most successfully destroy the tumor cells for each individual patient, leading to improved patient quality of life. One such therapy, AXL/STAT3 inhibition, shows great promise against aggressive tumors, not only in inhibiting tumor growth, but in affecting the entire tumor microenvironment.
Lung Cancer Drivers in Hispanic/Latinos
Dr. W. Douglas Cress is a Senior Member at the Moffitt Cancer Center.
Lung cancer by the numbers

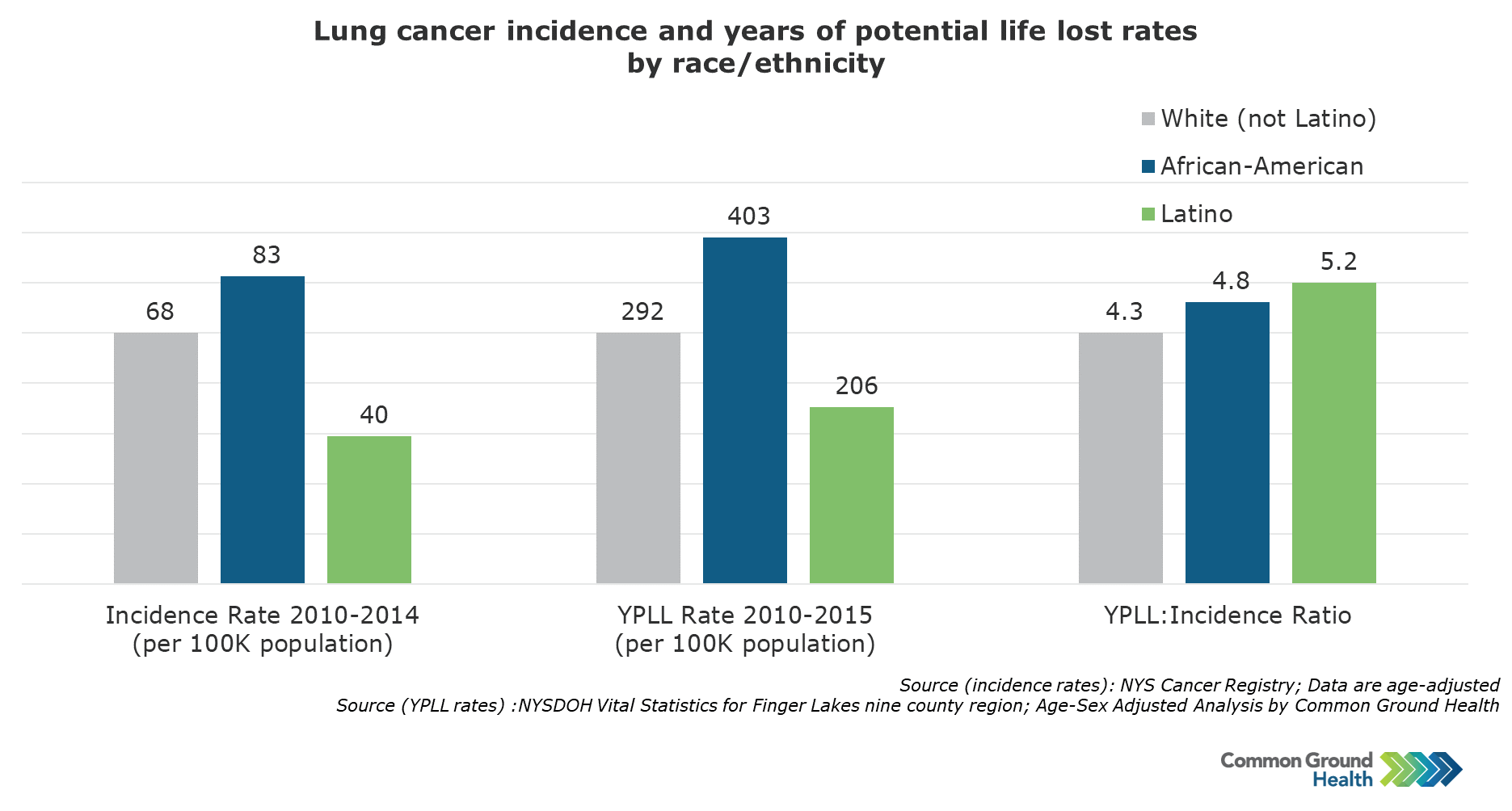
Lung cancer is the leading cancer killer of Latino men, and is second only to breast cancer in Latina women.1 Although Latinos have a lung cancer incidence rate of only 40 per 100,000, compared with 68 per 100,000 for the White population, Latino lung cancer patients die earlier than White patients, with 5.2 years of potential life lost compared with just 4.3 years for White patients.2 Dr. Douglas Cress seeks to address these troubling trends through his research on adenocarcinoma, one of the four major histological types of lung cancer (adenocarcinoma, squamous cell, small cell, and large cell). Adenocarcinoma is the most common histological type and represents 45% of all lung cancers.
Adenocarcinoma comes from type II pneumocytes, small cells in the lung that produce surfactants and participate in immune function. Two of the key driver mutations in adenocarcinoma are the EGFR and KRAS genes, which encode growth signaling molecules. The other three key driver mutations are in tumor suppressor genes: TP53, which is the guardian of the genome; KEAP1, which is involved in antioxidant protection; and STK11, which is involved in energy metabolism. When looking at The Cancer Genome Atlas (TCGA), a national cohort of mostly White participants, these five mutations account for a great deal of the disease. Among the patients in this cohort, 46% had a TP53 mutation, 33% had a KRAS mutation, 17% had a KEAP1 mutation, 17% had a STK11 mutation, and 14% had an EGFR mutation.3
A lung cancer cohort representing Latinos
Only 3% of TCGA participants, however, were Latino4, a population which is expected to represent a quarter of the US population by 2060. To address this disparity, Dr. Cress has been involved in the Puerto Rico Biobank, a core of the Ponce Health Sciences University and Moffitt Cancer Center U54 partnership to address cancer health equity. By partnering with the Oncology Research Information Exchange Network (ORIEN), the Puerto Rico Biobank has been able to contribute to the formation of a cohort similar to TCGA, but with a much greater Latino representation.
Lung cancer presentations unique to Latinos
When comparing this Hispanic cohort to TCGA, KRAS and STK11 mutations were found to be much lower in Hispanic patients, while TP53 mutations were found in similar numbers. EGFR mutations, however, were found in about 37% of Hispanics, compared with only about 15% of non-Hispanic White patients (P<0.001). Hispanic women had higher rates of EGFR mutations than Hispanic males (P<0.01), non-Hispanic males (P<0.01), and non-Hispanic females (P<0.001). EGFR mutations were also more common in non-smokers, a trend that was seen in both cohorts.5
Next, with the help of Dr. Julie Dutil, an expert in ancestry informative markers, the ancestry of the cohort participants was determined and divided into three groups: European, Indigenous American, and African. EGFR mutations were much more prevalent in the Indigenous American group than the European or African groups, an observation which has been noted among other researchers as well. Because of the small number of patients, the difference did not reach statistical significance. In a study of over 1000 participants from Latin America, Jian Carrot-Zhang and colleagues also found elevated EGFR mutations and decreased KRAS and STK11 mutations in Hispanic patients.6 To take ancestry into account, they calculated a local ancestry risk score showing that EGFR mutations were significantly positively correlated with Indigenous American ancestry (coeff.=0.55; 95%CI: 0.35-0.75; P=9 X 10-8).
A new finding in the Latino cohort
Dr. Cress closed by sharing about a project designed to examine the patients in the Latino cohort who did not have either EGFR or KRAS mutations. To this end, Dr. Cress performed Archer sequencing, targeted to identify fusion transcripts, on 55 tumors with no EGFR or KRAS mutations. Of the 55 tumors, 10 had unexpected novel fusions, 5 of which showed a fusion between ADCK4, a gene which encodes a protein involved in antioxidant metabolism, and NUMBL, a gene which encodes a protein involved in stemness. These two genes are very close together with only six kilobases between the two.
Research exploring the mechanism and prevalence of this fusion is already underway, but Dr. Cress and colleagues hypothesize that intergenic splicing of ADCK4 with NUMBL drives the expression of ADCK4-NUMBL chimeric transcripts. They also hypothesize that these transcripts express oncoproteins, and that these chimeras are expressed more frequently in Latino patients than in non-Hispanic White patients.
References
- American Cancer Society. Cancer facts and figures for Hispanic/Latino people 2018-2020. Accessed October 14, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-hispanics-and-latinos/cancer-facts-and-figures-for-hispanics-and-latinos-2018-2020.pdf
- Lung cancer incidence and years of potential life lost rates by race/ethnicity. Rochester, New York [cited 2022 Oct 3]. Available from: https://media.cmsmax.com/ravk3pgz5ktlujs1r08ci/lung-cancer-incidence-and-years-of-potential-life-lost-rates-by-race-ethnicity-finger-lakes-nine-county-region.png.
- Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature. 2014;511(7511):543-550.
- Spratt DE, Chan T, Waldron L, et al. Racial/ethnic disparities in genomic sequencing. JAMA Oncol. 2016;2(8):1070-1074.
- Gimbrone NT, Sarcar B, Gordian ER, et al. Somatic mutations and ancestry markers in Hispanic lung cancer patients. J Thorac Oncol. 2017;12(12):1851-1856.
- Carrot-Zhang J, Soca-Chafre G, Patterson N, et al. Genetic ancestry contributes to somatic mutations in lung cancers from admixed Latin American populations. Cancer Discov. 2021;11(3):591-598.
Feasibility and Acceptability of Culturally Adapted Survivorship Care Virtual Group Medical Visits (GMVs) for Spanish-Speaking Latinas with Breast Cancer in a Diverse Public Hospital Setting
As the most common type of cancer among Latinas, breast cancer produces a complex web of unmet needs in this community, both in terms of treatment and survivorship care. The more than 2.8 million breast cancer survivors in the United States face a risk of recurrence and secondary cancers, long-term adverse events from cancer treatments, difficulties in mental and sexual health, and challenges in access to preventive care, among other hardships.
Barriers to Effective Survivorship Care
Dr. Ana I. Velazquez of the University of California San Francisco and colleagues conducted a study evaluating group medical visits as a survivorship care strategy for Spanish-speaking Latinas who have survived breast cancer, and she presented her results on Wednesday, February 23, 2022, in the Rapid Fire Session. She began by detailing the complexities of breast cancer survivorship care and the need for access to cost-effective, comprehensive care that is both sustainable and high quality. To address the challenge of inefficient care delivery models, Dr. Velazquez and her group examined the feasibility and acceptability of culturally adapted GMVs, which have been used in other chronic diseases, as an avenue of delivering care for Latinas with breast cancer who speak Spanish.

The GMVs consisted of eight to ten patients meeting with providers on a weekly or regular basis for a total of four two-hour sessions. In each session, the patients received one-on-one time with the provider along with an hour-long lecture providing education surrounding the care of their chronic condition. These are billable healthcare appointments that allow more patients to be seen in a shorter amount of time.
Adapting the Survivorship GMV Model for Spanish-Speaking Latinas
A survivorship GMV model that had been implemented in an English-speaking population was culturally adapted to Latinas using a three-tier model. First, semi-structured interviews with patients and stakeholder meetings were conducted to set the stage. Second, modifications to the GMV model were made to create the initial adaptation, and primary and exploratory outcomes were selected. Third, the adapted survivorship GMV model was pilot tested and debrief sessions were carried out along with post-intervention surveys and semi-structured interviews. The primary outcomes were feasibility and acceptability of survivorship GMVs for Latinx patients with breast cancer, and the exploratory outcomes were knowledge, self-efficacy, and fear of cancer recurrence.
Acceptability and Feasibility of the Adapted Survivorship GMVs
Out of 17 patients enrolled, 15 (88%) attended all sessions, and the other 2 attended three of the four sessions. All were Spanish speaking with little to no English proficiency. When comparing the patient responses before and after the four GMV sessions, there was a substantial increase in the patients’ confidence regarding the following three statements: “I know what to expect now that my initial treatment is finished,” “I know how to take care of myself after cancer,” and “I will be able to give my primary care doctor details of my cancer treatment.” Although Dr. Velazquez and colleagues have not completed their analysis on all the qualitative data, the data they have so far indicate that their model is worth exploring as a method of increasing access to survivorship care for more patients.
The cost-effectiveness of GMVs as a healthcare delivery model, the relationship between GMVs and clinical and patient-reported outcomes, and the continuity and quality of survivorship care offered through GMVs need to be further evaluated in larger studies.
Social Determinants of Health Impact Gastric Cancer Risk in South Texas Minorities
Dr. Dorothy Long Parma, a physician from UT Health San Antonio, started her session with a discussion of how gastric cancer (GC) disproportionately affects the Latino community compared to non-Hispanic whites (NHWs). Disparities exist in both incidence and mortality, with the Latino risk of GC being at least twice that of NHWs. Furthermore, GC is the 6th and 8th leading cause of cancer death in Texas for Latino men and women, respectively. Among South Texas Latinos, multiple social determinants of health (SDoH) increase the vulnerability of this population to developing cancer.
Using Electronic Medical Records and the US Census to Build a Data Set

To examine the effect of ethnicity and SDoH on GC risk, Dr. Parma and colleagues used deidentified electronic medical records (EMRs) from adults 18 years of age or older diagnosed with GC and GC precursors on the Correa cascade at UT Health San Antonio and its safety net provider affiliate University Health System. The search for EMRs was done using ICD9/10 diagnostic codes and keywords. SDoH data was obtained from the American Community Survey and the US Census. With a sample size of 23,320, GC represented 2.6% (n=600) of the cases; more than half of the GC cases were male, and more than half were Hispanic; roughly 25% were on Medicare with about the same number privately insured. The result of the statistical analysis that followed shed light on certain factors associated with greater or lower risk of GC.
Higher Risk For Latinos and Lowest-Income Neighborhoods
According to Dr. Parma’s analysis, both Latino ethnicity and living in the lowest-income neighborhoods were associated with a higher risk of GC diagnosis (odds ratio [OR]: 1.24; 95% CI: 1.02-1.51; P=0.031 and OR: 1.3; 95% CI: 1.01-1.69; P=0.045, respectively). Interestingly, CareLink insurance, government insurance, being uninsured, and being underinsured all had lower odds of being diagnosed with GC compared with private insurance (OR: 0.31-0.56; all P<0.05), while military insurance was associated with an increased GC risk (OR: 2.67; 95% CI: 1.19-5.40; P=0.01). These numbers suggest a disparity in access to care between the Latino community and NHWs.
Insurance Barriers in the Latino Community
Using interaction models, the study revealed that Latinos without high school education had higher GC risk compared with Latinos with high school education (OR: 1.24; 95% CI: 1.10-1.52; P=0.04), and Latinos without insurance had higher GC risk compared with Latinos with insurance (OR: 1.16; 95% CI: 0.97-1.39; P=0.1). The “Other” category of race/ethnicity, including Asians, Native Americans, and those of multi-racial ethnicity, also showed an interaction with certain SDoH. Specifically, poverty and lack of insurance contributed to increased risk in this ethnic population (both P<0.05).
Dr. Parma concluded that minority groups with specific SDoH factors have increased GC risk compared with NHWs, and that solutions to overcome insurance barriers inhibiting early access to GC care should be actively pursued.
Cardiometabolic Comorbidities in Hispanic/Latino Cancer Survivors: Prevalence and Impact on Health-Related Quality of Life and Supportive Care Needs
Also in the Rapid Fire Session was Dr. Ashley Maras of the Feinberg School of Medicine, whose talk addressed the issue of cardiometabolic comorbidities in Hispanic/Latino cancer survivors and the associated health outcomes. Illness related to these comorbidities is the leading cause of death for cancer survivors treated for early-stage cancer, including prostate, breast, and colorectal cancers. Furthermore, these comorbidities are more prevalent in the Hispanic/Latino communities in the US compared with non-Hispanic whites (NHW). Overall, poor cardiometabolic health after cancer treatment is an issue in the Hispanic/Latino community that may have an effect on health-related quality of life (HRQoL), needs for supportive care, and health behavior changes.

Up to now, there has been a paucity of information concerning the prevalence of cardiometabolic comorbidities in Hispanic/Latino cancer survivors and the relationship between these comorbidities and health-related outcomes. More studies on these complex topics are likely to bring about better supportive care and improved HRQoL along with knowledge of specific survivorship needs and increased cardioprotective health behaviors.
Baseline Assessments of Hispanic/Latino Cancer Survivors with Cardiometabolic Comorbidities
Dr. Maras presented the results of a study in which participants, identified via medical chart review, were recruited from major tertiary centers in Chicago and San Antonio. Eligible patients had a diagnosis of breast, colorectal, or prostate cancer, had completed primary cancer treatment within the past 15 months, were self-identified as Hispanic/Latino, and were verbally fluent in Spanish or English. The baseline assessment measures included the Supportive Care Needs Survey (SCNS), the Functional Assessment of Cancer Therapy (FACT-G), the Charlson Comorbidity Index, the American Cancer Society (ACS) Lifestyle Behavior Scale, and electronic health records (EHR)-extracted medical/cancer information.
Sociodemographic Characteristics, Cardiometabolic Comorbidities, and Health Behavior Changes
The average age of the participants in the study was 56 years; 65.6% had an education level of high school or less; 68.4% had a household income of $50,000 or less; 59.4% were foreign-born; and 54.2% were monolingual Spanish-speaking. In terms of prevalence rates for cardiometabolic comorbidities, about one quarter of the patients had diabetes (compared to 10% in the general US population), about one fifth had peripheral vascular disease (compared to 4-10% in the general US population through age 79), and two to three percent had myocardial infarction, congestive heart failure, or stroke. The health behaviors that increased most commonly after a diagnosis of cancer were regular health check-ups, attempts to lose weight, and exercise.
Cancer Survivors With Cardiometabolic Comorbidities Versus Without
When compared to survivors without cardiometabolic comorbidities, those with cardiometabolic comorbidities reported lower overall HRQoL, functional wellbeing, emotional wellbeing, social wellbeing, and confidence in patient-provider communication (all P<0.05). In terms of supportive care needs, the survivors with cardiometabolic comorbidities reported greater unmet sexual needs (P=0.002). No differences were detected in increases in positive health behaviors between patients with and those without cardiometabolic comorbidities.
Dr. Maras speculated that the complexities of managing cardiometabolic comorbidities and cancer care contribute to the patients’ lack of confidence in communicating with providers, leading to unmet supportive care needs. She concluded by calling for more research and greater efforts toward the strategic development of intervention techniques to increase cardioprotective behaviors and improve outcomes for Hispanic/Latino cancer survivors with cardiometabolic comorbidities.
Cultural Differences in Family Caregiver Support in End-of-Life Cancer Care
Dr. Paul Maciejewski is Associate Professor of Biostatistics in Radiology at Weill Cornell Medicine as well as Co-Director of the Cornell Center for Research on End-of-Life Care.
Advanced care planning

Because of the breadth of information involving the role of caregivers and end-of-life care, Dr. Maciejewski chose to focus his presentation on family influences on advanced care planning (ACP) among patients with advanced cancer. ACP is a process that enables patients to make plans regarding future medical care that may include discussions about end-of-life (EoL) care and completion of advance directives. Benefits of ACP include less frequent receipt of intensive, unbeneficial, burdensome care coupled with more value-concordant care; earlier hospice referrals; less suffering and loss of dignity; and better quality of death. Unfortunately, there is disparity in ACP, with Latino patients less likely to engage in ACP than non-Latino patients.
Understanding ACP in Latinos
In order to further understand this disparity, Dr. Maciejewski and colleagues began the Coping with Cancer III study, comparing ACP and end-of-life care in Latinos and non-Latinos. This study, sponsored by NIH Minority Health and Health Disparities, set out to determine if religious, familial, and cultural beliefs mediate or moderate disparities in ACP and EoL care. It was a multi-site, prospective cohort study of advanced cancer patients, their family/informal caregivers, and their oncology providers with recruitment sites in New York City, Chicago, Dallas, El Paso, and Miami.
The study included patients with advanced lung, gastrointestinal, and gynecological cancers and their informal/family caregivers. Among these patient/caregiver dyads, 57 were Latino, and 90 were non-Latino White, totalling 147 dyads. The study outcomes focused on aspects of ACP such as patient EoL discussions with oncologists and completion of advance directives (e.g., do-not-resuscitate (DNR) orders, living wills, and healthcare proxies). Variables of interest included caregiver ethnicity, relationship to patient, and cultural attitudes and beliefs, as well as patient consultation with family members about important medical decisions.
Disparities in Latino patients and caregivers
Both Latino patients and caregivers were more likely to be younger, live in lower income households, and be less well educated when compared to non-Latinos, although patients were equally likely to be married. Latino patients were also less likely to complete DNR orders, have living wills (LWs), or have designated healthcare proxies (HCP). Latino caregivers were less likely to be spouses or partners of patients and more likely to be adult children of patients. These adult child caregivers were more likely to live with the patient in the Latino cohort, at 65%, while only 10% of non-Latino adult child caregivers lived with the patient.
Patient consultation with family members
When considering patient consultations with family members about medical decisions, Latino and non-Latino patients were equally likely to discuss important medical decisions with spouses, adult children, parents, and siblings. Among Latinos, however, patients who had consulted with a parent were five times more likely to have a DNR than not. Further, if a Latino patient consulted with a parent or sibling, they were more likely to designate a HCP. These findings, together with the fact that parents and siblings are less likely to be primary caregivers, indicate that discussion with loved ones who are not the primary caregiver increases the likelihood of a DNR order and the designation of an HCP.
Four critical cultural beliefs
Latino caregivers were found to be more likely to value four cultural attitudes: fatalismo, familismo, machismo, and respeto. Fatalismo is the belief that events are beyond one’s control, familismo involves dedication and loyalty to family, machismo is a sense of masculine pride, and respeto indicates a deferential respect of the medical care system. All of these beliefs, in particular fatalismo and machismo, may prevent ACP in patients and caregivers. The Coping with Cancer Care III study showed that caregivers of patients without a DNR order or HCP displayed greater fatalismo, machismo, and respeto. All four beliefs were also stronger in caregivers of patients without LWs.
In summarizing his conclusions, Dr. Maciejewski emphasized the evidence of ethnic disparities in ACP. He also noted that Latino caregivers were less likely to be spouses and more likely to be adult children. While Latino and non-Latino patients were equally likely to discuss important medical decisions with family members, among Latino patients, consulting with parents was associated with more DNRs and more HCPs. Finally, certain cultural beliefs (fatalismo, machismo, respeto) were stronger in Latino caregivers and associated with fewer advance directives (DNRs, LWs, HCPs).
Gastrointestinal Cancers in Latinos: Recent Trends and Emerging Risk Factors
Dr. V. Wendy Setiawan is the Jane and Kris Popovich Chair in Cancer Research and a professor of population and public health sciences at Keck School of Medicine of the University of Southern California (USC).
A closer look at liver and pancreatic cancer

For her presentation, Dr. Setiawan chose to focus on two cancers which are important in the Latinx population: liver and pancreatic cancer. Among Latinx patients, the most prevalent GI cancers are colorectal, liver, and pancreatic cancer in men; and colorectal and pancreatic cancer in women. Liver and pancreatic cancer are among the top six cancer killers in Latinx men and among the top seven cancer killers in Latinx women. Although mortality rates for colorectal cancer and stomach cancer have decreased in the general population over the past three decades, liver and pancreatic cancer mortality rates have increased in both men and women.
Liver cancer in the Latinx community
In Dr. Setiawan’s own large, prospective, multi-ethnic cohort study, Latinos had the highest incidence rates of liver cancer compared to other ethnic groups. Furthermore, the study examined whether generation status among Mexican Latinos influenced risk of liver cancer. The population was divided into four groups: immigrants born in Mexico with Mexico-born parents, US-born first-generation residents with Mexico-born parents, US-born second-generation residents with one parent born in Mexico, and US-born second-generation residents with both parents born in the US. Compared to Mexico-born participants, all US-born participants had a higher risk of liver cancer. The risk was highest among the second-generation residents with both parents born in the US. Birthplace, however, was a more predictive risk factor for liver cancer than generation status.
Metabolic syndrome and NASH
Other risk factors for liver cancer include Hepatitis B and C, excessive alcohol intake, and metabolic syndrome. Non-alcoholic steatohepatitis (NASH), the liver manifestation of metabolic syndrome, is the most severe form of non-alcoholic fatty liver disease (NAFLD), and incidence of NASH-related liver cancers in the US increased eightfold between 2002 and 2016. By contrast, alcohol-related liver cancer rates were quite stable. Although chronic hepatitis C remains the leading etiology for liver cancer in White patients, NASH recently surpassed chronic hepatitis C as the leading etiology for liver cancer in Latinx patients. Accordingly, population-attributable risks suggest that eliminating diabetes would have the highest impact in terms of liver cancer prevention in the Latinx community.
Factors contributing to the progression of fatty liver or NASH to liver cancer are also important to identify. A recent study using data from 270,000 participants from the Department of Veterans Affairs (VA) identified factors associated with disease progression to liver cancer: age, obesity, Hispanic ethnicity, cirrhosis, hypertension, dyslipidemia, obesity, and diabetes. Diabetes, hypertension, dyslipidemia, and obesity showed a stepwise increase in liver cancer risks with each additional metabolic trait, with diabetes conferring the highest risk of progression to liver cancer among patients with fatty liver.
Pancreatic cancer in the Latinx community
Although cancer death rates in the US have been declining from 1994 to 2018, pancreatic cancer death rates have steadily increased, and the disease is predicted to become the second leading cause of cancer death after lung cancer. Since 1994, early onset pancreatic cancer incidence has increased much more in Hispanic and non-Hispanic White women compared with men, while late onset pancreatic cancer has increased at approximately the same rate in both genders.
Known risk factors for pancreatic cancers include cigarette smoking, chronic pancreatitis, family history of pancreatic cancer, obesity, and diabetes. In fact, more than 50% of pancreatic cancer cases are diagnosed within three years of a diabetes diagnosis. This is an important finding because diabetes is prevalent in both African American and Latinx populations, although pancreatic cancer risk is higher among African American communities.
Dr. Setiawan summarized her presentation by reiterating that Latinx patients are at increased risk of liver cancer. Evidence also suggests that early onset pancreatic cancer is increasing in Latinx women. With NASH becoming the most common underlying etiology of liver cancer in Latinx patients and diabetes greatly increasing pancreatic cancer risk, global awareness about metabolic risk factors is needed. Furthermore, more research must be conducted to identify high risk populations for both diseases, and screening protocols must be updated to increase the chances of early detection.
Explore More:
CancerBy The Numbers
142
Percent
Expected rise in Latino cancer cases in coming years


{kind=link}