
Share On Social!
COVID-19 can affect anyone.
But, in reality, it’s worsening the health and social inequities facing U.S. Latinos.
Now the pandemic is raising fears of racial/ethnic and income disparities in coronavirus exposure, testing, prevention via social distancing, and treatment.
“As the number of cases rises, citizens are rightfully concerned about who is getting tested and who will receive treatment,” writes health equity adviser Brian Williams in a column for the Dallas Morning News. “For those who exist on the margins of health care justice, access to life-saving treatment is never guaranteed.”
Disparities in Coronavirus Exposure
We know Latinos are more likely than their white peers to suffer from poverty, underlying conditions, and a lack of quality housing and transit. They also are more likely to work lower-wage jobs—custodians, construction or fast food workers, package handlers.
This makes them disproportionately vulnerable to COVID-19 exposure and infection, WHYY reports.
Is that playing out in the data?
So far, yes, for African Americans, ProPublica reports.
“Cities and states tracking COVID-19 cases by race have shown that African Americans are disproportionately affected than other races,” they report. “[This] has also led to a high mortality rate due to environmental, economic, and political factors that can weaken lungs and make immune systems vulnerable.”
 What about Latinos?
What about Latinos?
About 16% of U.S. Latinos who say they were infected with COVID-19, had been in contact with someone who was infected, or knew someone who was infected, compared with just 9% of whites, according to a Reuters/Ipsos survey.
Also, Ibram X. Kendi, director of The Antiracist Research and Policy Center, explored coronavirus rates and racial makeup by zip code in New York City (29% Latino).
In the city’s most-infected zip code, 37% are Latino.
In the second-most, 64% are Latinos.
“Averaging out the racial composition of the five New York City zip codes with the highest coronavirus rates shows a significant overrepresentation of Latinos (45.8 percent) and Asians (23.4 percent), and a significant underrepresentation of whites (21.2 percent) and blacks (8 percent) when compared with their citywide populations,” Kendi wrote for The Atlantic.
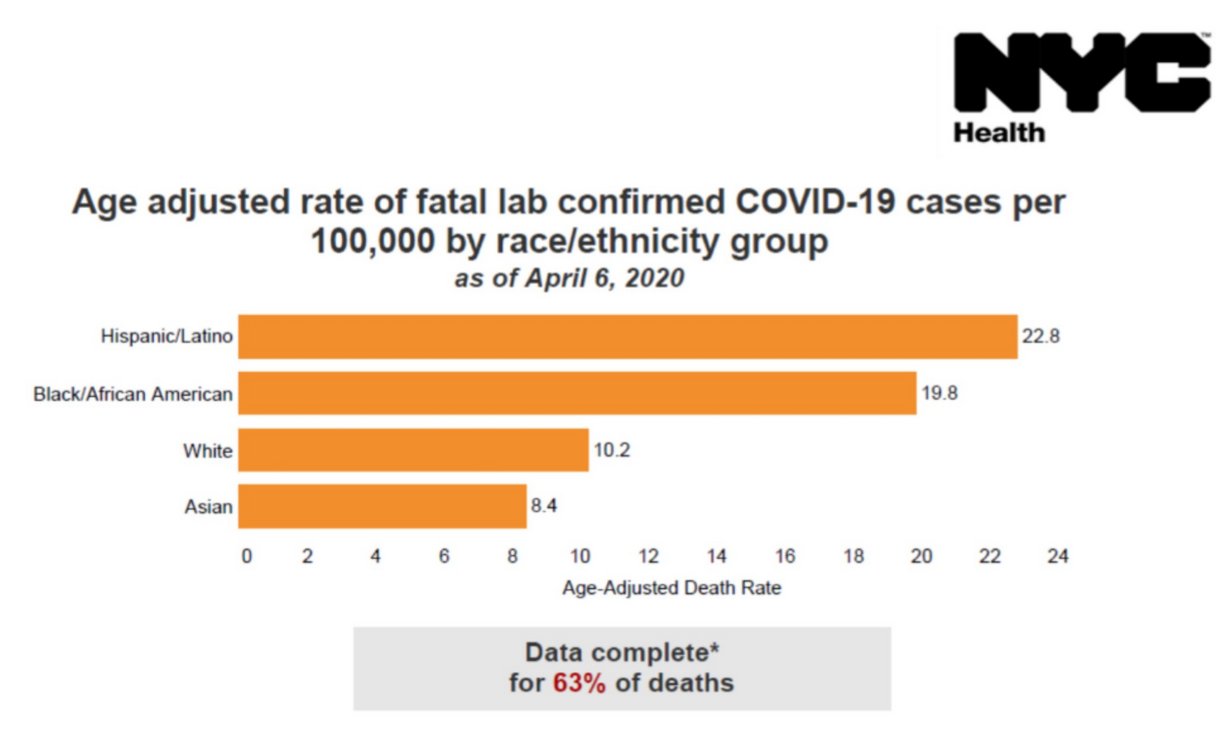 New NYC data released on April 8, 2020, seem to confirm this.
New NYC data released on April 8, 2020, seem to confirm this.
The age-adjusted death rate for COVID-19 is 22.8 per 100,000 people among Latinos in New York. This is higher than the rate among African Americans (19.8), whites (10.2), and Asian Americans (8.4).
Disparities in Coronavirus Testing
In Philadelphia (15% Latino), people who live in higher-income neighborhoods have gotten tested for the coronavirus six times more frequently than those in lower-income areas.
This is “social inequality,” says Usama Bilal of Drexel University, the man behind the data.
Those who have health insurance get tested for coronavirus more frequently than those who don’t, even though you don’t have to have insurance to get tested, Bilal told the Philadelphia Inquirer. Often it takes having a car to get in line for drive-through testing.
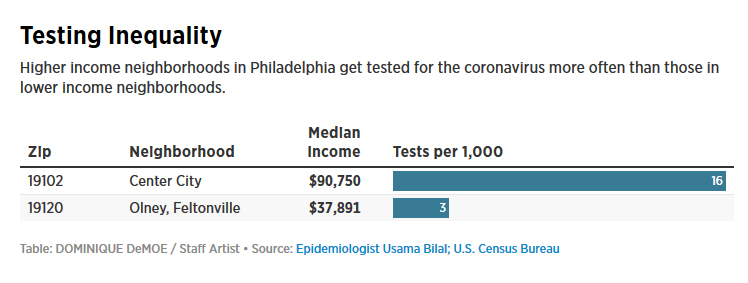 So it’s not surprising he found that areas with the highest concentrations of Latinos, who have low access to health insurance and personal cars, had the fewest tests.
So it’s not surprising he found that areas with the highest concentrations of Latinos, who have low access to health insurance and personal cars, had the fewest tests.
“Because low-income people are preoccupied with keeping their jobs at a time of soaring high unemployment, Bilal said, it’s possible they’re not thinking about testing,” according to the Inquirer. “Also, many low-income Philadelphians work at jobs that don’t offer sick pay, and they might not be able to afford to miss work for a test. Ultimately, Bilal said, ‘lots of people are asymptomatic and opt to work over getting tested. The fatality rate of the virus is not as high as the 100% fatality rate of not eating.'”
A group of lawmakers recently sent a letter to Health and Human Services Secretary Alex Azar asking for race-inclusive data in coronavirus testing, AP News reports.
“Any attempt to contain COVID-19 in the United States will have to address its potential spread in low-income communities of color, first and foremost to protect the lives of people in those communities, but also to slow the spread of the virus in the country as a whole,” they wrote.
“This lack of information will exacerbate existing health disparities and result in the loss of lives in vulnerable communities.”
Disparities in Coronavirus Prevention for Social Distancing
Not everyone can practice social distancing, even if they want to.
“Not only are essential workers more likely to be exposed to the virus on the job, they are also less likely to be able to take the recommended social distancing measures to prevent getting infected, or to be able to self-isolate if they do get the virus,” WHYY reports.
 This could make it harder for residents in low-income neighborhoods to keep their distance, Sharrelle Barber, an epidemiologist at Drexel University, told WHYY.
This could make it harder for residents in low-income neighborhoods to keep their distance, Sharrelle Barber, an epidemiologist at Drexel University, told WHYY.
“Not only is the individual themselves at risk, but now their families are at risk, and perhaps folks in their communities,” Barber said. “We can see how, as this pandemic unfolds over time, it not only puts individuals within marginalized racial groups at risk, but whole communities.”
Some even call social distancing a privilege.
“Staying at home is a privilege. Social distancing is a privilege. The people who can’t must make terrible choices: Stay home and risk starvation or go to work and risk contagion,” wrote Charles M. Blow in The New York Times. “People can’t empathize with what it truly means to be poor in this country, to live in a too-small space with too many people, to not have enough money to buy food for a long duration or anywhere to store it if they did.”
Disparities in Coronavirus Prevention for Wearing Medical Masks
When social distancing can’t be maintained, CDC now recommends people wear “cloth face coverings in public settings.”
 But medical masks are in short supply. Many have to make their own.
But medical masks are in short supply. Many have to make their own.
Covering the face with a bandanna, scarf, or T-shirt is often associated with gang affiliation, crime, or violence. Many don’t feel safe wearing these in place of masks, according to Fernando Alfonso III of CNN.
“On social media and in interviews with CNN, a number of people of color — activists, academics and ordinary Americans — expressed fears that homemade masks could exacerbate racial profiling and place blacks and Latinos in danger,” wrote Alfonso.
That can make masks a lose-lose situation for people of color, ReNika Moore of ACLU told CNN.
“Not wearing a protective bandana goes against CDC recommendations and increases the risk of contracting Covid-19, but wearing one could mean putting their lives at risk of getting shot or killed because of racially-biased targeting,” Moore said.
Disparities in Coronavirus Treatment
Treatment is increasingly important amid emerging disparities in coronavirus exposure and testing.
COVID-19 can severely affect people who have underlying conditions. Cancer patients and people with heart disease or diabetes, for example.
At the same time, the pandemic also is likely to cause a shortage of hospital beds, ICU beds, and ventilators, according to researchers writing in the New England Journal of Medicine.
 Who decides who gets what resources?
Who decides who gets what resources?
Public health leaders worry about how racial bias in medicine could affect the care people receive.
Studies show that doctors—especially white doctors—have implicit, subconscious preferences for white patients over those of color. Latino men, for example, are less likely to get treatment for high-risk prostate cancer than white men.
Not to mention Latino immigrants, who bear the brunt of an anti-immigrant society.
“[In the pandemic] we may see racialized patterns of survival based on the choices that doctors … have to make about who lives and who dies,” Barber told WHYY.
Can We Try to Ensure ‘Fairness’ in Allocating Medical Resources?
The same researchers who expect coronavirus to cause a shortage of hospital beds and ventilators offer six recommendations to stay ahead of the curve:
Maximize benefits. “Priority for limited resources should aim both at saving the most lives and at maximizing improvements in individuals’ post-treatment length of life,” the authors wrote. “Limited time and information in a Covid-19 pandemic make it justifiable to give priority to maximizing the number of patients that survive treatment with a reasonable life expectancy and to regard maximizing improvements in length of life as a subordinate aim.”
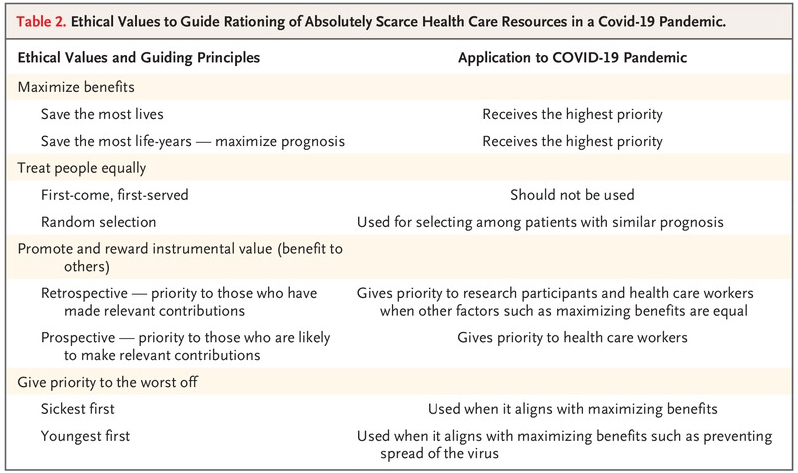 Prioritize health workers. “These workers should be given priority not because they are somehow more worthy, but because of their instrumental value: they are essential to pandemic response. If physicians and nurses are incapacitated, all patients … will suffer greater mortality and years of life lost.”
Prioritize health workers. “These workers should be given priority not because they are somehow more worthy, but because of their instrumental value: they are essential to pandemic response. If physicians and nurses are incapacitated, all patients … will suffer greater mortality and years of life lost.”
Do not allocate on a first-come, first-served basis. “For patients with similar prognoses, equality should be invoked and operationalized through random allocation, such as a lottery, rather than a first-come, first-served allocation process,” the authors wrote. “Treatments for coronavirus address urgent need, meaning that a first-come, first-served approach would unfairly benefit patients living nearer to health facilities. And first-come, first-served medication or vaccine distribution would encourage crowding and even violence during a period when social distancing is paramount.”
Be responsive to evidence. “Federal guidance currently gives priority to health care workers and older patients, but reserving some tests for public health surveillance (as some states are doing) could improve knowledge about Covid-19 transmission and help researchers target other treatments to maximize benefits.”
Recognize research participation. “People who participate in research to prove the safety and effectiveness of vaccines and therapeutics should receive some priority for Covid-19 interventions. Their assumption of risk during their participation in research helps future patients, and they should be rewarded for that contribution.”
Apply the same principles to all Covid-19 and non–Covid-19 patients. “There should be no difference in allocating scarce resources between patients with Covid-19 and those with other medical conditions. If the Covid-19 pandemic leads to absolute scarcity, that scarcity will affect all patients, including those with heart failure, cancer, and other serious and life-threatening conditions requiring prompt medical attention.”
The authors suggest that these six recommendations can help create fair guidelines.
“Such guidelines can ensure that individual doctors are never tasked with deciding unaided which patients receive life-saving care and which do not. Instead, we believe guidelines should be provided at a higher level of authority, both to alleviate physician burden and to ensure equal treatment.”
Will This ‘Fairness’ in Allocating Medical Resources Work Equitably?
Some warn that “fairness” may not be the right word.
“Prioritizing some lives means not prioritizing others. Deciding who lives is also deciding who dies. As the conversation around this becomes more prevalent, don’t use euphemisms like ‘fair,'” writes Joelle Marie for The Mighty. “Don’t try to gloss over the reality.”
In the end, most public health leaders agree on one thing.
The pandemic — both viral and of fear — will magnify the large inequities that exist in our society and have major implications for health, said Ana V. Diez-Roux of Drexel University.
“Some of us have access to quality health care, but others do not. Some of us have paid sick leave, but others do not,” said Diez-Roux. “Some of us get paid even if our employer closes down for a couple of weeks, but others do not. Some of us have other health conditions that make us more vulnerable, but others do not. Some of us can easily work from home, but others cannot.”
Explore More:
AccessBy The Numbers
142
Percent
Expected rise in Latino cancer cases in coming years


